


What Patient H.M. Taught Us About Memory
Henry Molaison’s anterograde amnesia offered never-before-seen neurobiological insights into how our memories are created

Before diving into Patient H.M.’s case, let’s understand how memories work first…
Our brains are actively forming new memories, strengthening or retrieving existing ones, and consolidating learned information every single day. And different types of memory, both by duration and content, correspond with distinct regions of the brain. We have short-term and long-term memory, explicit (declarative) and implicit (non-declarative) memory. These different types of memory often interact and complement each other, and can be strengthened mainly through repetition and active recall — among other methods.
Despite this, our memory is fragile. It is very susceptible to error in not just injured, but also healthy brains.
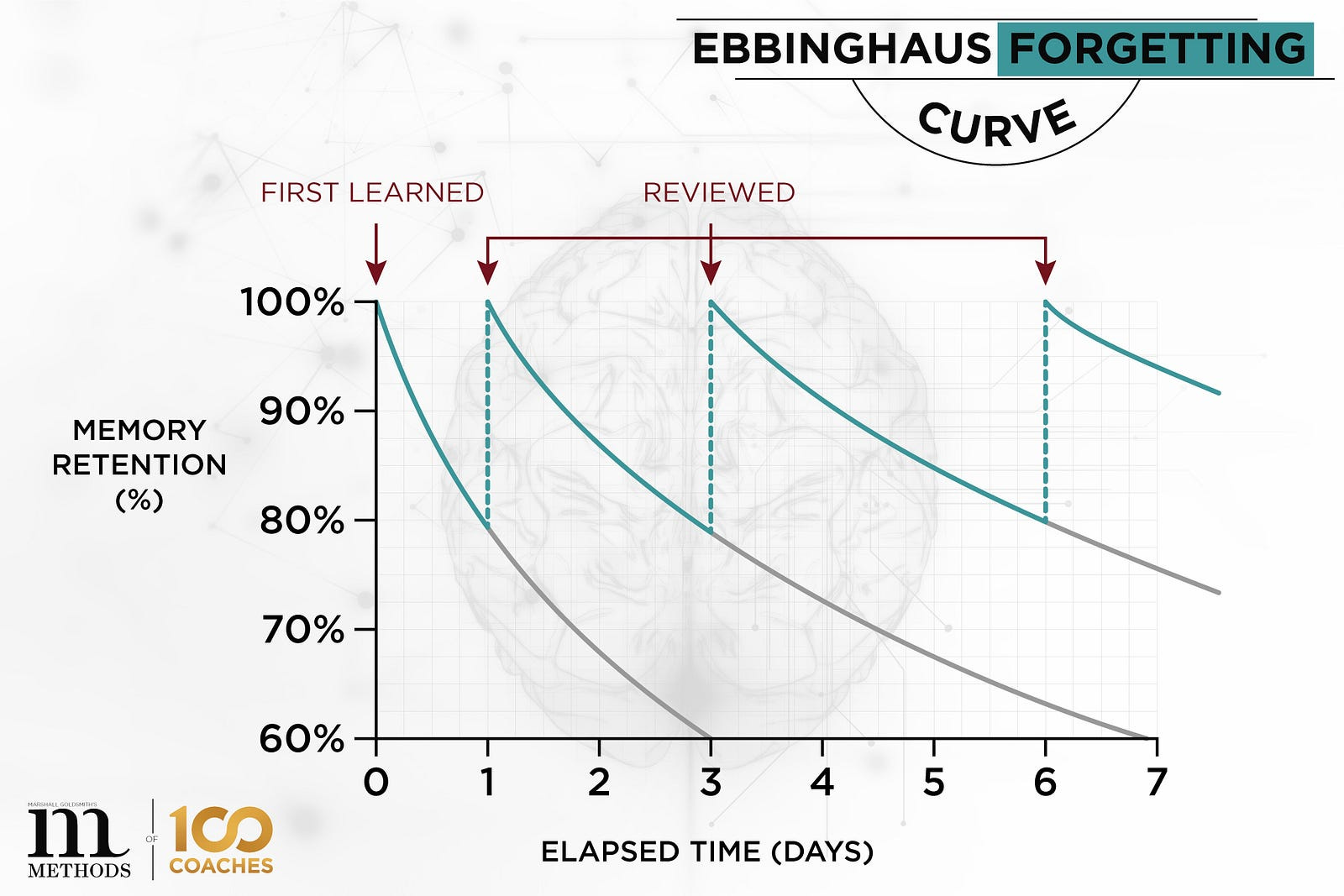
As seen above in the Ebbinghaus Forgetting Curve, a large part of the memories we form tends to be forgotten rapidly within just a few days. It is because of this that a lot of our memories are — at least to some extent — flawed. This is simply the nature of how our brains store and retrieve memories. Everything in biology and nature comes at a cost — the currency of which is energy — and the same applies to storing memories. We can’t store 100% of our memories 100% of the time. As much as the human brain is unimaginably complex and capable, it has been evolutionarily designed to prioritize what information to retain and what to get rid of over time to ensure efficiency. Of course, there are other factors involved such as a failure to retrieve info, weak initial encoding of info, and commonly, a phenomenon called interference in which we tend to forget things when remembering something else.
That said, as shown in the Ebbinghaus curve once again, through active recall and repetition we can enhance our memories and delay forgetting them quite substantially the more we review. Reviewing leads to changes in the synaptic strength of networks between neurons that underlie long-term memory, strengthening them over time. It is because of this that, in reviewing for an exam for instance, it is much more effective to space out studying over several days than to cram.
Memory comes in three main stages you may have heard before: Encoding, Storage, and Retrieval. It is through these three stages that all our memories are made and ultimately remembered.

A breakdown of the stages of memory:
Encoding: A subset of the sensory information that enters the sensory buffers is encoded and placed into the short-term memory (STM).
Storage: If the information is rehearsed or used, it may consolidate into long-term memory (LTM), lasting from minutes to a lifetime.
Retrieval: When we probe memory, individuals retrieve information from LTM and place it into STM for use.
Now let’s learn some neuroanatomy…
Medial Temporal Lobe
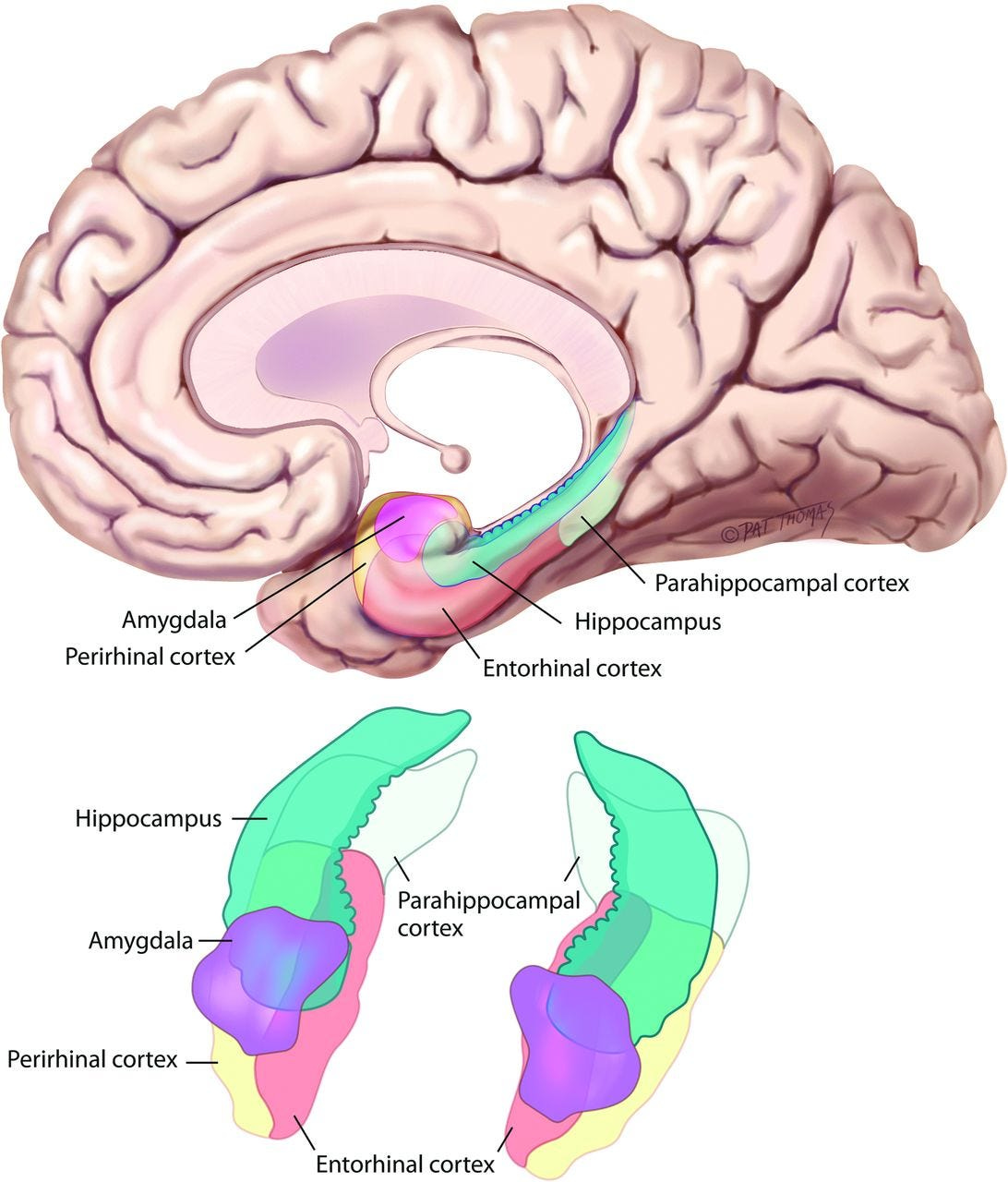
This region of the brain plays a crucial role in forming memories, navigation, and the perception of time — all of which are crucial in the development of long-term declarative memory. It is the region in which the three stages of memory primarily take place and is one of the centres of the brain with the highest and most complex levels of cognitive activity. The medial temporal lobe consists of the following cortical and subcortical structures:
Entorhinal cortex: this region of the brain connects the hippocampus to the neocortex — the site of higher cognitive functioning in the cerebral cortex — and is involved in encoding and transferring declarative memory, as well as spatial navigation information, between the two structures. (think of this cortical structure as an interface between the place where memory is encoded, the hippocampus, and the place where memory is stored and can be retrieved from, the neocortex)
Parahippocampal gyrus: this cortical structure in the medial temporal lobe is responsible for making sense of spatial memory and navigation. Located directly adjacent to the hippocampus, the parahippocampal gyrus is a hub that combines sensory information to create a cohesive picture of the surrounding environment and the memories associated with it.
Hippocampus: seahorse-shaped subcortical structure nestled deep in the medial temporal lobe that mediates the conversion of short-term declarative memory into long-term declarative memory and also plays a big role in processing spatial relationships.
The Hippocampus in greater detail
Going back in our evolutionary history, we may have originally had the hippocampus for spatial navigation but then co-opted it for remembering life events — a theory attributed to neuroscientist John O’Keefe and his colleagues.
How did we discover the hippocampus’ role in spatial navigation?
Through maze experiments done on rats. When a rat is in a particular location in a maze, specific hippocampal neurons fire at each location — this seems to be how the rat seems to keep track of where it is in space. What happened when the hippocampi were lesioned? The rats became disoriented and weren’t aware of their surroundings nor could they remember how to navigate the maze successfully (check out the water maze done by Hollup et al., 2001b).
The cells responsible for conveying this spatial info are called hippocampal place cells, which fire specifically when you’re in a certain place. It’s extraordinary that these cells can create cognitive maps using various modes of sensory info and specific firing patterns that paint a picture of your environment, or “place field”.

How Memory is Formed on a Synaptic Level through Plasticity
Memory storage requires physical changes to the synaptic connections of the brain. Following a training period, synapses may be modified in several ways…either:
More neurotransmitters are released presynaptically.
There is a higher sensitivity to neurotransmitters postsynaptically (by an increase in receptors on the postsynaptic cell for instance).
Increased size of synapse presynaptically, postsynaptically, or both.
Input from other neighbouring neurons may cause extra depolarization or hyperpolarization at the axon terminals, causing changes in the amount of neurotransmitter released at the synapse. With these changes in neurotransmitter release, memories can be established by strengthening synaptic connections.
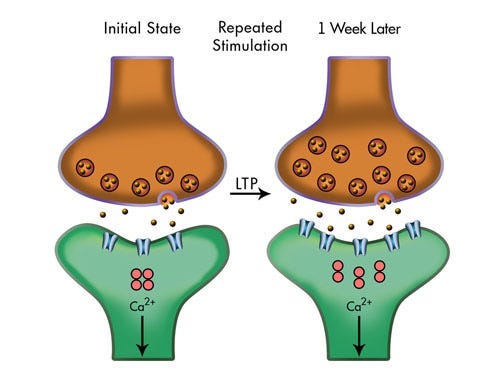
As when exercise tones muscles, sometimes communication between two cells becomes significant enough to require the formation of additional synapses. If one pathway becomes more active relative to another due to repeated stimulation, the more active pathway takes over sites previously occupied by the less active pathway — a process that can lead to long-term potentiation (LTP). LTP increases the efficiency of neurotransmission in the more active pathway, which leads to the strengthening of the associated memory.
I’ll talk a lot more about memory on the synaptic level and particularly LTP in my next article :)
Memory by Content
There are multiple types of memory, and each one has a specific role in how we process and recall information. Facts and generic knowledge, such as “Brussels is the capital of Belgium,” are stored in semantic memory, while prior life experiences and events are stored in episodic memory. Both semantic and episodic memory are considered different forms of explicit memory.
The cerebellum and basal ganglia, two centres of the brain critical to movement and coordination, are involved in skill learning — also known as procedural or implicit memory, which includes learning motor skills and other behaviours. Stimuli and responses are linked in classical conditioning — a type of non-declarative memory — frequently without the subject’s conscious knowledge.
In addition, priming is used to describe the subconscious impact of prior experiences on our subsequent ideas or behaviours, whereas spatial memory allows us to navigate places and recall locations. Together, these different types of memory cooperate to enable us to properly move around and comprehend the world.
The Case of Henry Molaison
Little did he know he would accidentally spur a revolution in our understanding of human memory and its organization
Henry Molaison was an American man from Manchester, Connecticut who lived between 1926 and 2008. He began to have epileptic seizures when he was 10, which worsened throughout his teens and 20s until his seizures became so incapacitating by age 27 (in 1953) that he underwent bilateral medial temporal lobectomy to relieve it — a surgical procedure that was done to remove his medial temporal lobes. Often regarded as the most famous patient in the history of neuroscience research, his unique condition allowed scientists to understand learning and memory on another level.
Dr. William Scoville performed a bilateral medial temporal lobectomy on H.M., removing his hippocampi and its nearby structures in an attempt to cure Henry’s debilitating seizures. His seizures decreased; memory, however, was impaired. Patient H.M.’s IQ was 104 before surgery, but strangely soared to 118, meaning that his intellect was above average. He generally had normal perceptual and motor abilities but was left with very poor memory → mild retrograde amnesia and couldn’t form new episodic memories ever again → severe anterograde amnesia.
Now that’s pretty serious! Henry could never recognize the people who studied him for 30 years, would always be surprised it was not 1953, and no matter how much time passed, he was surprised that he wasn’t still 27.
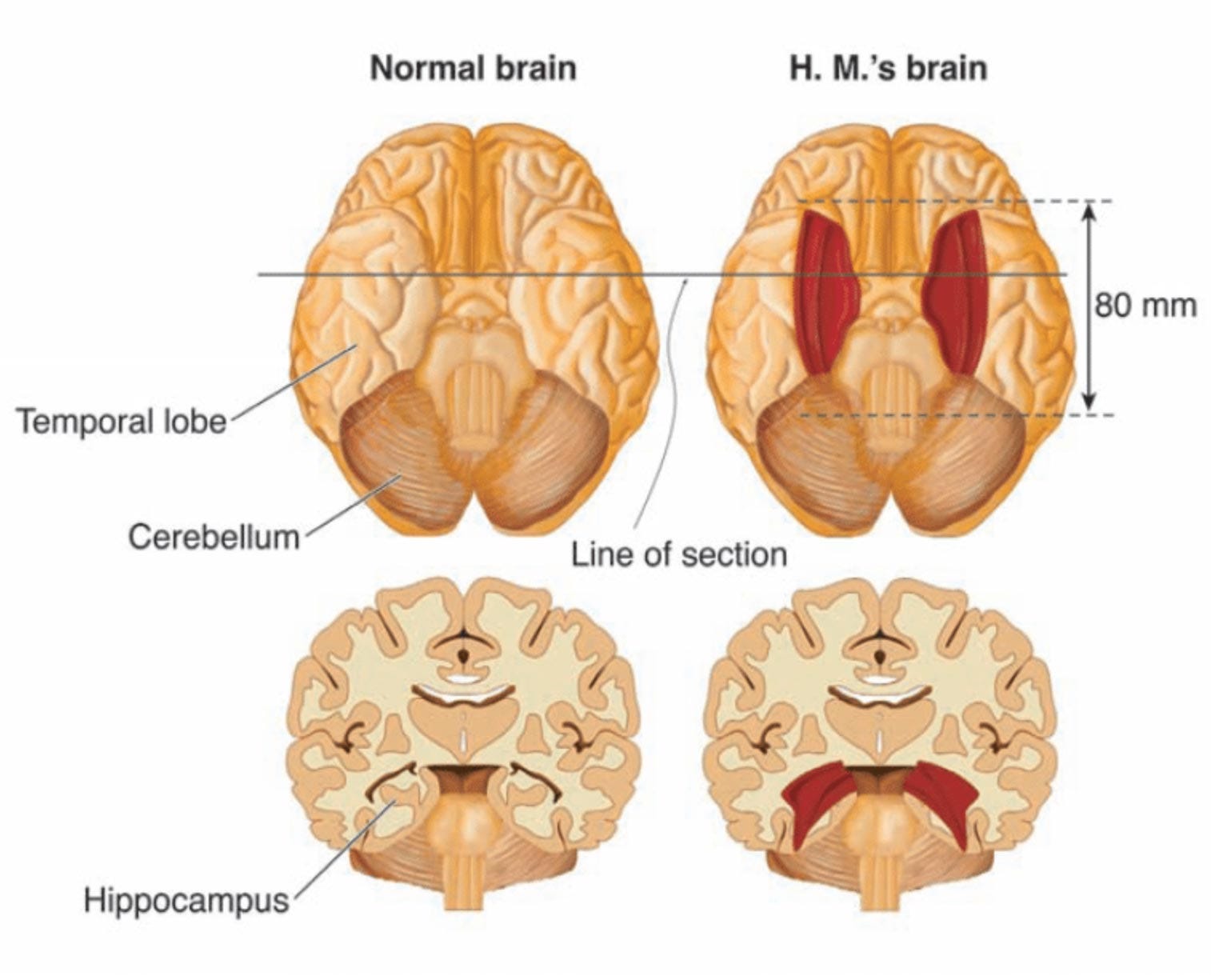
The reason that H.M. could remember much of the events in his past, is that those memories had already been encoded and stored in his neocortex previously. Following the lobectomy, however, he could not encode any new memories with the loss of his hippocampi and associated structures like the entorhinal cortex and parahippocampal gyrus. The loss of his medial temporal lobe was the reason for his complete anterograde amnesia — a significant discovery that researchers who went on to study him for over 50 years made.
But, what could H.M. do?
British-Canadian neuropsychologist Dr. Brenda Milner and Dr. William Scoville (who performed the lobectomy on Henry) organized a series of tests for H.M. to perform to assess his short-term and long-term memory. He was able to remember a list of 6–7 digits on the Digit Span +1 test, which is within the usual range for most people. In a similar vein, he performed within the normal range on the Block-Tapping Memory Span test, which involves tapping a series of blocks in the right order. These results imply that H.M. was able to temporarily store and manipulate knowledge because his working memory and short-term memory systems were still largely operational.
The Mirror-Drawing Task
H.M.’s capacity to pick up new motor skills was evaluated in addition to his short-term and working memory assessments, particularly in the Mirror-Drawing Task. Because of the reversed visual feedback, this exercise presents a substantial challenge as participants must trace a figure while only gazing at it in a mirror. Over several training sessions, H.M.’s performance on this task consistently improved, which indicated normal sensory-motor learning despite his severe anterograde amnesia. The areas of his brain that were involved in procedural memory and motor learning appeared to be intact, as evidenced by his capacity to get better with repeated practice.
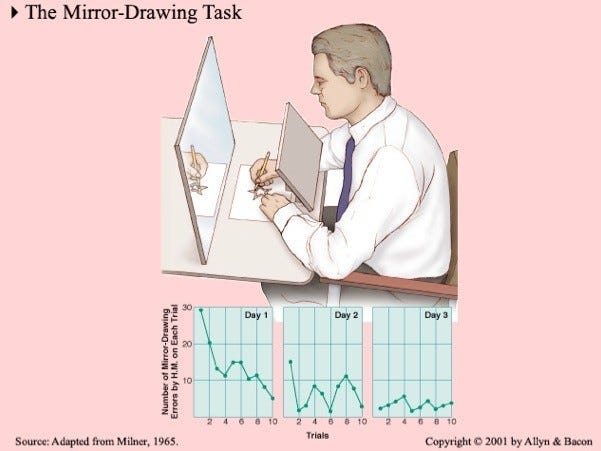
Dr. Milner and Dr. Scoville pointed out that H.M. had no conscious recollection of completing the assignment, demonstrating the dissociation between his retained capacity to pick up new skills and his incapacity to recall the events involved in that learning. This discovery provided concrete evidence in favour of the theory that different neural networks in the brain underlie different forms of memory, including declarative and procedural memory.
Patient H.M. also did activities like the Rotary-Pursuit Test, in which his performance increased with repeated training sessions like in the Mirror-Drawing Task. In the Rotary-Pursuit Test, Henry showed the capacity to pick up new behavioural abilities, suggesting typical sensory-motor acquisition. Although he had no conscious memory of the words from the original list, he also had normal priming — a propensity to use words heard recently more readily. H.M. could not even remember completing the task itself, but he was able to master conditioning tasks like Pavlovian conditioning, where repeated training enhanced his performance.
Despite these skills, the removal of H.M.’s medial temporal lobe structures ultimately made it virtually impossible for him to form and use explicit memories when he had to map new knowledge.
What has Patient H.M. taught us?
H.M.’s case study completely revamped our understanding of the neurobiology of memory. His condition led to the discovery that implicit and explicit memory rely on separate but parallel neural systems and that the hippocampus is essential for the consolidation of episodic memories, among other things. Having been extensively tested for 50+ years, patient H.M.’s legacy will live on as the most studied person in neuroscience. What’s sad, though, is that he taught us about our memory only by losing his own.